Dr. Miller Featured in Plastic Surgery Practice

The role of volume augmentation for facial rejuvenation will continue to progress as our knowledge and insight into facial anatomy, aging, beauty, and aesthetic harmony continue to mature. Soft-tissue augmentation has been used with positive results for some time, but the focus within the facial aesthetic community, as a whole, of where to place volume has certainly changed and expanded. With experience, practitioners recognize that filling just a wrinkle or nasolabial fold, for example, can help or, better yet, appease a patient's concern, but true facial rejuvenation, with harmony, requires a more thoughtful scope of evaluation and an expanded treatment philosophy.
Treating the Hallow Temples
The hollow temple is an area often overlooked by patients and practitioners alike. Once pointed out, the expression is one of surprise for not recognizing this obvious "problem" before. Or if previously known, hairstyles have commonly been changed or altered to conceal the area. The lack of fullness within the temple area can be due to a relatively deep temporal fossa, a hypoplastic temporalis muscle, or an atrophied adipose tissue layer.
Most temples do have a slight concavity, but too much concavity (or convexity) disrupts the frame or silhouette of the face. The hollowness also exposes the superior-lateral orbital ridge and zygomatic arch, which are features deemed less attractive and associated with aging and/or poor health. Consequently, the aim in treating the hollow temple is to provide a better overall shape to the face and a smooth transition from the peri-orbital area to the temporal hairline.
Figure 1 is a 5-year follow-up photograph of a patient with fat augmentation to the peri-orbital area (tear trough and infra-brow) and cheeks. The improvement and longevity from her fat-augmentation procedure is evident, but if you now evaluate and consider the temple area, the results become less impressive. No fat was placed in her temples, and the resulting hollowness, over time, accentuated her superior-lateral orbital rims and provided a less than ideal appearance and facial shape.
Another example of the importance of temple augmentation is illustrated in Figure 2. This 63-year-old female underwent a high-superficial musculoaponeurotic system (SMAS) facelift, fractional CO2 laser resurfacing, and fat augmentation. From her preoperative photograph to postoperative year 1, her temples are satisfactorily filled from her fat-augmentation procedure despite being on a significant weight loss program. A 25-plus-pound weight loss during year 2 recreates the hollowness once corrected by fat augmentation. Notice the improvement in her facial shape and overall peri-orbital aesthetics when her temples are revolumized or "rescued" with hyaluronic acid (HA) fillers.

For the hollow temples, the most common treatment methods are fat augmentation, poly-l-lactic acid (PLLA), and syringe-based fillers such as HA fillers. The benefits, longevity, and techniques of fat augmentation to the temples and other facial areas are well established. Fat augmentation is often combined with other facial aesthetic surgery procedures, including brow lifting, but the procedure may have limitations for some patients. Commonly, patients with very deep hollowed temples, who are seeking aesthetic improvements, are patients with very limited fat stores.

In these circumstances, the fat stores may be either too limited for any fat-augmentation procedure or only enough fat exists for transfer to more aesthetically "vital" areas, such as the peri-orbital or cheek areas. Additionally, fluctuating weight, which significantly impacts transplanted adipose cells, as illustrated above in Figure 2C, and downtime can be significant deterrents for some patients.
For these reasons, PLLA and HA fillers are excellent alternatives. PLLA's safety profile and its effects on temple (and overall facial) augmentation are well established.2 The volumizing from PLLA comes from the induction of fibroplasia (collagen growth), which in reality takes multiple treatments and months for the results to present themselves fully. This can be seen as an advantage because many patients like the idea of temple filling with their own "collagen," and the slow progression to end result provides privacy. Friends, family, and co-workers will not see a dramatic overnight change in their appearance. The results begin to diminish by 2 years, but much longer outcomes are not uncommon.
Fat Augmentation Versus PLLA for Temple Augmentation
The technical aspects between fat augmentation and PLLA are significant. For instance, fat is typically placed throughout the subcutaneous and temporoparietal fascia layers where the facial nerve resides, and down to but superficial to the deep temporal fascia layer. In contrast, the needle or cannula delivering PLLA is placed through the deep temporal fascia and then deep to the temporalis muscle onto the temporal fossa bone(s), where a small depot of PLLA is deposited. It is noteworthy to mention that the temporal fossa is, indeed, covered with a thin, adherent periosteum (pericranium). The point is significant for two reasons.
Many physicians recall that the periosteal layer of the scalp transitions to become the deep temporal fascia layer, which covers the temporalis muscle, without recognizing that a portion does extend on the undersurface of the temporalis muscle to cover the temporal fossa.3,4 Without periosteum, there would be a limited supply of fibroblasts to manufacture collagen. The fibroplasia in this plane acts like a shim elevating the temporal contents.
However, despite the deep placement, some amount of fibroplasia can be seen (during brow lifts) and felt (with needle resistance in subsequent PLLA treatments) in the more superficial layers. The basis is presumably from the permeability of the deep temporal fascia as well as PLLA seeping through the penetration sites made in the deep temporal fascia upon injection, and facilitated further by the massage regimen encouraged after the procedure. The reasons for the deep placement were from complications with nodules and papules reported in the temporal area when more concentrated and superficial placements of PLLA were reported.5,6
Treating Hollow Temples with HA-BASED Fillers
The "latest" treatment for temple filling is with HAs such as Restylane or Juvéderm. In contrast to placement in lips or nasolabial folds, these fillers are hydrated with saline and/or lidocaine.7 The reasons for this are at least twofold. Hydration allows more volume of product (albeit at lower density and tonicity), and promotes smoother placement of product. The hydration also decreases the risk of the Tyndall effect (bluish discoloration). The placement is in the more "elastic" subcutaneous layer and approximates the temporoparietal fascia layers. Thus, the volume expansion is often more substantial than what is seen with PLLA. One reason for this is anatomical. The deep temporal fascia is a relatively thick, durable fascia layer attached firmly at its edges on bone (temporal line of fusion, processes of the lateral orbital rim, zygomatic arch).
Like a moderately tight drum, volume augmentation underneath the fascia has a limited capacity to distend or elevate, especially more superior in the temple where the deep temporal fascia is a single layer.8 Consequently, hyaluronic fillers are an ideal treatment for hollow temples because of their more superficial placement and can be offered to patients as a stand-alone procedure or as a supplement to fat augmentation or PLLA treatments.
The technique of hollow temple filling with HA is straightforward. Typically, patients will require a minimum of 2 cubic centimeters (cc) of HA filler per side. Hydration volumes vary, but adding 3 cc of bacteriostatic saline (0.9%) and 1 cc of 1% or 2% lidocaine (with or without epinephrine) is sufficient. This provides 6 cc of volume and will fit in most 5-cc syringes.
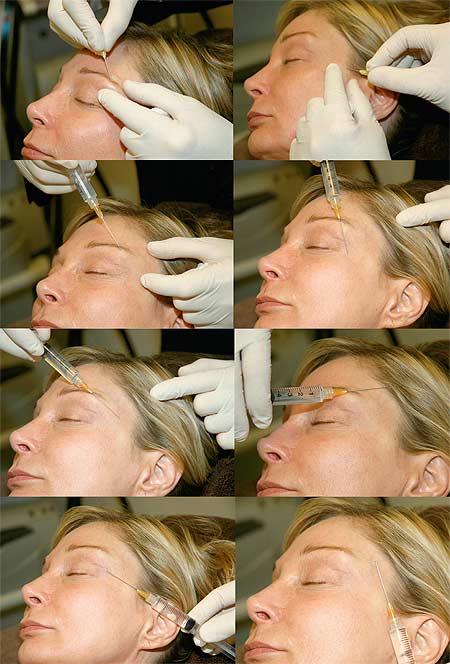
I use a disposable 25-gauge 1.5-inch cannula (DermaSculpt, CosmoFrance Inc, Miami, or a 0.7 Tulip infiltrating cannula (Tulip Medical Products Inc, San Diego) for placement. Initial entrance sites (usually two to three) are made using a small needle (20 to 23 gauges). The product is then delivered in a threading fashion using a slow, controlled fanning motion.

Cross hatching over areas ensures a smooth and consistent result (Figure 4). Much of the edema will dissipate in minutes to hours as the saline and local anesthesia is absorbed. Follow-up in 3 to 4 weeks is standard, allowing more filler placement if required (Figure 5).
The risks associated with any temple-augmentation procedure should not be minimized. Injury to the facial nerve is possible and is one of the reasons that cannulas are used in fat grafting and during HA filler placement. Other risks include hematoma, vessel occlusion or emboli, numbness, infection, and the occasional superficial vessel in the temple becoming more prominent after filler placement. The vessel usually returns back to its normal size in hours but can persist for 2 to 3 weeks.
The hollow temple is an additional area that should be examined for patients seeking facial rejuvenation. The hollow temple often goes unrecognized and untreated, but several safe and effective treatment options are available.
To schedule your personal consultation with Dr. Miller, please call 949-482-1752. You can also request your consultation online.